

Ijraset Journal For Research in Applied Science and Engineering Technology
Comparative Effect of Faradic and Russian Currents on the Quadriceps Muscle in Patients with Knee Osteoarthritis
Authors: Neha Rani, Sonam Verma, Karishma Das, Palas Pramanick, Komal Chauhan
DOI Link: https://doi.org/10.22214/ijraset.2023.55301
Certificate: View Certificate
Abstract
Osteoarthritis is amongst the most common musculoskeletal condition which affects overall function and quality of life in the Indian population. Clinical features of knee osteoarthritis include pain that affects the functional mobility of joints and thus interferes with walking and activities of daily living. Quadriceps function declines with age, and is further impaired in patients with knee and may contribute to the risk of falls. The aim of the present study was to compare the effect of Faradic and Russian Currents on the quadriceps muscle in Patients with knee osteoarthritis. Objectives: To evaluate the effect of Faradic Currants on the quadriceps muscle for the management of knee osteoarthritis. To evaluate the effects of Russian Currants on the quadriceps muscle for the management of knee osteoarthritis. To Comparative effects between Faradic and Russian Currants on the quadriceps muscle for management of knee osteoarthritis. Methodology: Permission from the head of the department of Sanskriti University Mathura, and approval from the ethical committee. Patients pre-diagnosed with grade II OA were selected for this study. Consent was taken from the patients after confirming the diagnosis of Grade II OA. The subjects were divided into two groups (15 in each group): one group consist of a Faradic current + quadriceps isometric exercise (5 days a week for 4 weeks) and the second group consisted of a Russian current + quadriceps isometric exercise (5 days in a week for 4 weeks). Result: The statistics are done based on the objectives and hypotheses and it has been organized by following three sections: Section I: Frequency and percentage distributions of socio-demographic variables. Section II: Effectiveness of pre and post-test values. Section III: Comparison of Faradic Currants and Russian Currants Values. Conclusion: This study concludes that faradic current and Russian current show significant effect in quadriceps muscle in patients with knee osteoarthritis and there is no significant difference between faradic and Russian current on quadriceps muscle Patients with knee osteoarthritis. But the only significant difference in WOMAC scores after intervention (The WOMAC score is more decreased in Russian as compared to faradic current)
Introduction
I. INTRODUCTION
Knee osteoarthritis (OA) joint disease commonly occurs in the elderly population and it causes significant pain and functional limitations [1]. OA is classified into Primary OA and Secondary OA. Primary OA occurs as a result of natural wear and tear of knee joint structures due to aging, overuse, or obesity, whereas Secondary OA occurs due to known primary causes like trauma, infection [2]. The Kellgren and Lawrence scale classifies OA into four grades as follows: Grade 0 indicates no radiographic findings of OA; Grade 1 indicates minimum osteophytes of doubtful clinical significance; Grade 2 indicates definitive osteophytes with unaffected joint space; Grade 3 indicates definitive osteophytes with moderate joint space narrowing; and Grade 4 indicates definitive osteophytes with severe joint space narrowing and subchondral sclerosis [3]. Pathologically it is characterized by focal loss of articular hyaline cartilage with the proliferation of new bone at the margins, subchondral sclerosis, and remodelling of joint contour [4].
The earliest symptom of OA knee is pain. Patients also complain of crepitus, stiffness, and swelling of the joint. On examination, tenderness along the joint line, terminal limitation of movement, weakness, and atrophy of the quadriceps femoris muscle. The radiographic features of OA knee include narrowing of joint space, osteophyte formation, loose bodies, and subchondral sclerosis [5]. Joint space narrowing occurs due to the erosion of the cartilage as part of the degenerative process associated with arthritis but the best method of evaluating the progression of the cartilage destruction is through measurement of joint space width [6].
A recent survey in India reported that the prevalence of OA in older adults more than 65 years of age was 32.6% in the pastoral population and 60.3% in the urban population [7]. Men are affected more commonly than women [8].
Various measures are available for the treatment of OA knee such as conservative management including pharmacotherapy (NSAIDS, Corticosteroid therapy), physiotherapy, and surgical management [5]. Manual therapy, physical therapy modalities, taping techniques, patient education and therapeutic exercises, and orthosis are all used to treat knee OA [9].
According to the World Journal of Orthopedics 2011, isometric exercises are helpful in improving muscle function. Exercises such as static Quadriceps, static hamstrings, strengthening the vastus medialis, mini squats, use of Quadriceps table, and 10 to 15 repetitions, done 5 days a week for 2 weeks have proved to be effective in improving muscle strength [10,11]. Quadriceps femoris muscle plays an important role in the mechanics of the knee joint [12]. It is the only muscle crossing anterior to the axis of the knee and is the prime mover for knee extension. During the quiet standing and stance phase of gait, the knee is an intermediate joint in a closed chain.
The quadriceps muscle controls the amount of flexion at the knee during initial contact and also causes knee extension through reverse muscle pull on the femur during mid-stance. It also controls the amount of flexion during pre-swing (heel off to toe off) and excessive heel rise during an initial swing. With the loss of quadriceps function, the patient lurches the trunk anteriorly during initial contact to move the center of gravity anterior to the knee so that it is stable or rotates the extremity outward to lock the knee; with fast walking there may be extreme heel elevation during initial swing [13].
Russian current is a medium-frequency current. Russian current was developed for upgrading muscle strength in Russian Olympic athletes and was found to increase force earn up to 40%. Russian current is an Alternating Current modulated sinusoidal with 2500- Hz transfer in a series of bursts (a 10-millisecond burst and a 10-millisecond interval). It has been reported that the most commonly used electric stimulation to increase muscle strength, reduce pain and improve physical function in Russian current [14].
Neuromuscular stimulation may be an alternative approach for muscle-strengthening training programs. Faradic current may be the better mode of electrical stimulation to boost muscle strength and muscle mass. Voluntary muscle contraction followed by the faradic current may result in functional faradism at the same time.
The functional paradigm is an essential portion of neuromuscular stimulation which can be useful in boosting muscle mass and strength of muscle and improving functional mobility in knee OA.
To improve the muscle strength and size of muscle fiber, each contraction of the muscle followed by faradic stimulation simultaneously may be a better and more useful rehabilitative way of knee OA. Although previous studies found improvement in muscle mass, strength of muscle, and function after the implementation of faradic current stimulation [15]. Surged faradic current is used for upgrading muscle strength and vascularity of muscle [16]
A. Purpose of the Study
Many Previous studies investigated the effectiveness of Russian current and also faradic current on the quadriceps muscle in Patients with knee osteoarthritis but no comparative study was performed between the effect of faradic and Russian current on the quadriceps muscle for the management of knee osteoarthritis. So this study will conduct to examine the Comparison between the effect of faradic and Russian current on the quadriceps muscle for the management of knee osteoarthritis.
B. Significance of the Study
This study will be conducted to find out the comparative effect of Russian and faradic current for the management of OA knee this study will be beneficial to create better physiotherapy treatment protocols for the management of OA knee and this study aims to provide important information about the management of OA and to impart knowledge.
C. Aims of the Study
To find out the Comparison between Faradic and Russian Currants on the quadriceps muscle in Patients with knee osteoarthritis.
D. Objectives
- To evaluate the effect of Faradic Currants on the quadriceps muscle for the management of knee osteoarthritis.
- To evaluate the effects of Russian Currants on the quadriceps muscle for the management of knee osteoarthritis.
- Comparative effects between Faradic and Russian Currants on the quadriceps muscle for management of knee osteoarthritis.
E. Research Hypothesis
- Null Hypothesis (H0): There will be no significant difference between Faradic and Russian current on the quadriceps muscle in patients with knee osteoarthritis.
- Experimental Hypothesis (H1): There will be a significant difference between Faradic and Russian current on the quadriceps muscle in patients with knee osteoarthritis.
II. MATERIALS & METHODOLOGY
- Sample Size: 45 subjects (3 groups and 15 subjects in each group)
- Data Collection: Data collection were done from SCPM Medical College Haripur road gonad.
a. Inclusion Criteria
- Pre-Diagnosed case of Grade II OA patients
- Age: 45-60yr
- Gender: Both male & female
- Complaining of knee pain that has lasted longer than 3 months,
- A pain level that is medium
b. Exclusion Criteria
- Any recent hip or knee surgeries & fractures Patients with neurological deficit
- Soft tissue injuries of lower limb
- Any systemic illness
III. VARIABLES
A. Dependent
- NPRS (Numeric pain rating scale),
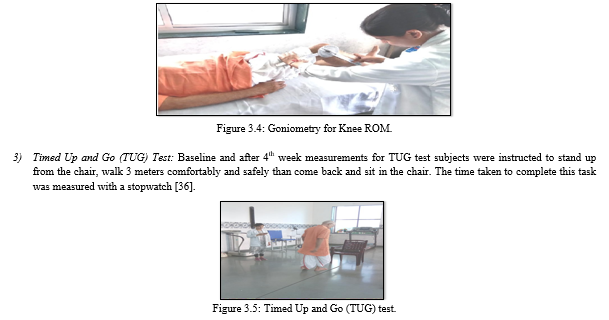
- Goniometric measurement for ROM of knee,
- Timed Up and Go (TUG) test,
- Western Ontario and McMaster Universities Osteoarthritis Index
B. Independent
- Faradic current
- Russian current
IV. INSTRUMENTATION
- A stopwatch
- Standard Chair with arm rest
- Universal Goniometer
- Weighing machine
- A stadiometer
- Couch
- Electrical stimulation machine having Faradic Current
- Electrical stimulation machine having Russian Current
A. Procedure
A total of 30 subjects were enrolled in this study. Both males and females participated in this study for 45 -60 years. The subjects were made to sign the informed consent form before the study. The consent form was explained in a language which comfortable for the patient. 30 subjects were randomly selected in the treatment groups (Group A&B) by simple random sampling by chit-picking method on the basis of inclusion and exclusion criteria. Participant‘s demographic data was collected including their body weight in kg measured by using the weighing machine, Height in cm measured by using the stadiometer and Participant‘s BMI which is in Kg/m2 was calculated using the participant's weight and divided by the square of the appropriate height.
Baseline measurements for pain intensity by NPRS, knee ROM by goniometer, Timed Up and Go (TUG) test, and WOMAC were taken for every patient after that faradic current + Quadriceps isometric was applied for group A and Russian current + Quadriceps isometric was applied for group B than post-intervention outcome measures were taken at the end of 4th week.

V. BASELINE AND POST-INTERVENTION MEASUREMENTS PROCEDURE
1) NPRS (Numeric Pain Rating Scale): Baseline and after 4th-week measurements for knee pain intensity by NPRS in which asked the patients to select the numerical value of the scale i.e. range 0-10 and express verbally which indicates about his/her pain intensity [18].
2) Range of Motion of Knee: Baseline and after 4th-week measurements for active range of motion of the knee was measured by a universal goniometer and recorded in degrees. These measurements were taken for knee flexion and knee extension. According to Norkin & White when measuring knee flexion the patient was placed in a supine lying with the knee extension. Position the hip in 0 degrees of extension, abduction, and adduction. The femur Stabilization was done to prevent rotation, abduction, and adduction of the hip. The testing position was to hold the anterior thigh with one hand and the ankle with the other hand Move the patient‘s thigh to approximately 90 degrees of hip flexion and move the knee into flexion. To prevent further hip motion stabilize the thigh and guide the lower leg into knee flexion. When resistance is felt the end of the range of knee flexion occurs. Goniometer placement was the fulcrum placed over the lateral epicondyle of the femur, the Stationary arm with the lateral midline of the femur, using a greater trochanter as a reference, and the movement arm with the lateral midline of the fibula, using the lateral malleolus and fibular head as a reference and during measurement of knee extension the patient placed in supine lying. A folded towel is placed under the ankle to ensure that the knee is in full extension. The femur Stabilization was done to prevent rotation, abduction, and adduction of the hip. Goniometer placement in knee extension measurement is the same as knee flexion [34]
4) WOMAC Arthritis Index: The Western Ontario and McMaster Universities Arthritis Index was done before (pre) and after (post) the intervention, including five response levels for each item, representing different degrees of intensity (none, mild, moderate, severe, or extreme) that was scored from 0 to 4. The pain dimension or scale includes five items asking about pain at activity or rest. The stiffness dimension includes two questions. The function dimension explores the degree of difficulty in 17 activities. The final score for the WOMAC was determined by adding the aggregate scores for pain, stiffness, and function. Scores range from 0 to 96 for the total WOMAC where 0 represents the best health status and 96 the worst possible status. The higher the score, the poorer the function. Therefore, an improvement was achieved by reducing the overall score [37]
VI. INTERVENTION
- Group A: Faradic current + quadriceps isometric exercise (5days in a week for 4 week)
After taken the baseline measurement of the patient we started the intervention of the patients who are randomly selected in group A than applied the faradic current after the resting period of 10 min following quadriceps isometric exercise. For faradic stimulation the patient were placed comfortable in supine lying position on a couch with pillow placed below the knee joint adequate positioning of standard carbon rubber electrodes of equal paired size were placed on the quadriceps muscle of the arthritic knee joint .the electrodes was securely fixed using Velcro strap and set the electrical stimulation intensity which was set at the maximum tolerance of the patient. Parameters included rectangular biphasic symmetric current, pulse duration of 400 μs and stimulation frequency of 80 Hz. The session was given for 10 min and was comprised of 10 s of stimulation followed by 20 s of rest for 5 days/week for 4 weeks. For quadriceps isometric exercise Patients were in supine position with legs straight with the towel roll placed under the knee, patients were asked to press the knee on the towel roll. This exercise aimed to strengthen quadriceps muscle. The patient was instructed to maximally activate their thigh muscles in order to straighten their knee. This exercise was of 3 sets of 10 repetitions each for 5 days/week for 4 weeks (20 days).

2. Group B: Russian current + quadriceps isometric exercise (5days in a week for 4 week).
After taken the baseline measurement of the patient we started the intervention of the patients who are randomly selected in group B than applied the Russian current after the resting period of 10 min following quadriceps isometric exercise. For Russian stimulation the patient were placed comfortable in supine lying position on a couch with pillow placed below the knee joint adequate positioning of standard carbon rubber electrodes of equal paired size were placed on the quadriceps muscle of the arthritic knee joint .the electrodes was securely fixed using Velcro strap and set the electrical stimulation intensity which was set at the maximum tolerance of the patient. Russian Current of 2500 Hz with pulse frequency of 50 Hz, symmetric pulses of sinusoidal form, with a pulse duration of 200-300 μs, 2-3 seconds ramp up, 2 seconds ramp down for comfort and a duty cycle of 50% was applied for 10 minutes duration for 5 days/week for a period of 4 weeks after that instructed the patient to quadriceps isometric exercise. This exercise was of 3 sets of 10 repetitions each for 5 days/week for 4 weeks.

VII. DATA ANALYSIS
Analysis was done for 30 subjects who completed the study. The outcome variables of the study included Knee pain intensity on NPRS, Knee range of motion by Goniometry, TUG and WOMAC.
Paired t-test was used for comparing the pretreatment and post-treatment scores of each variable for both the groups (within group analysis). Independent t-test was applied to compare the outcome values between the group A and group B. The value of all two groups i.e. Group A (Faradic current) and Group B (Russian current), were compared at the pre test and after 4th Week of treatment.
Statistical significance was set at P < 0.05. P value > 0.05 was considered as non significant difference while P value < 0.05 was considered to have represented a significant difference. Value of confidence interval was set at 95%.
A. Result
The statistics done based on the objectives and hypotheses and it has been organized by following three sections.
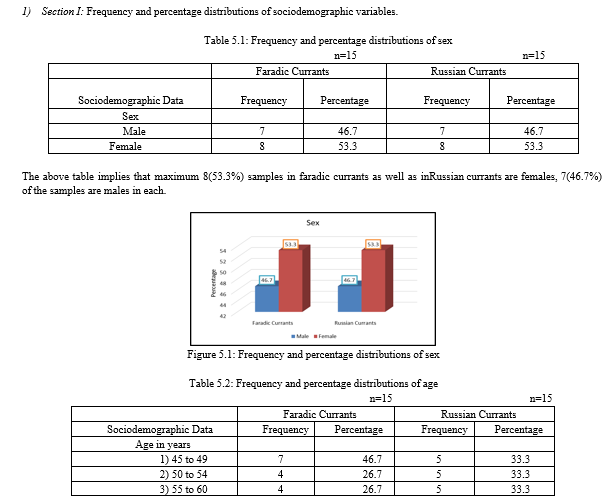
- Section I: Frequency and percentage distributions of sociodemographic variables.
- Section II: Effectiveness of pre and posttest values.
- Section III: Comparison of Faradic Currants and Russian Currants values
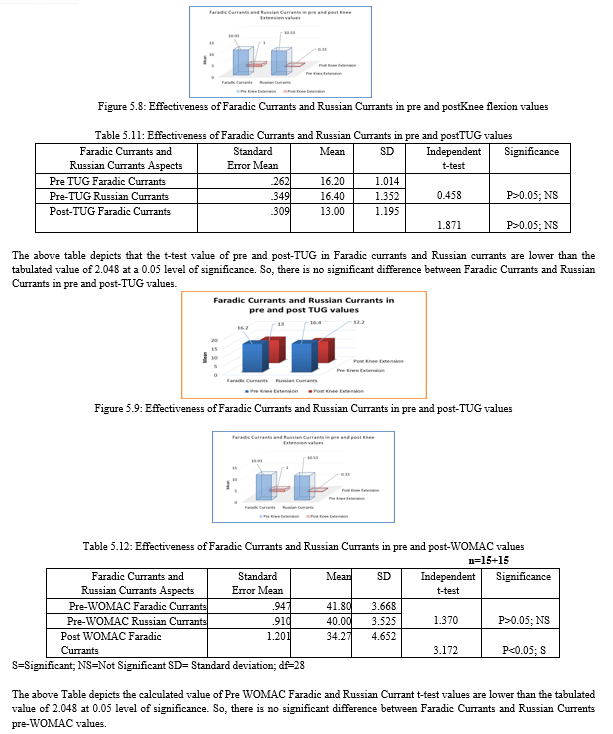
In the Post WOMAC Faradic Currants and Post WOMAC Russian Currant t-test values are higher than the tabulated value 2.048 at 0.05 level of significance. So, there is a significant difference between Faradic Currants and Russian Currants WOMAC values.
VIII. DISCUSSION
The study was designed to determine the effect of Faradic and Russian currents on the quadriceps muscle in patients with knee OA. The purpose of the study was to compare the effect of Faradic and Russian currents on quadriceps muscle in patients with knee OA in order to increase ROM of the knee, decrease pain and improve functional ability of knee joint. The findings of this study are based on the objectives and hypotheses and it has been organized by following three sections.
- Section I: Frequency and percentage distributions of Sociodemographic variables.
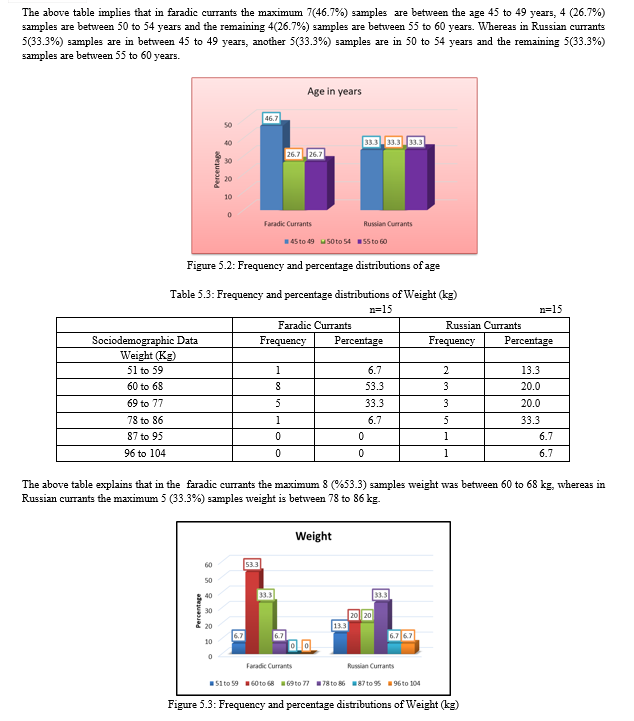
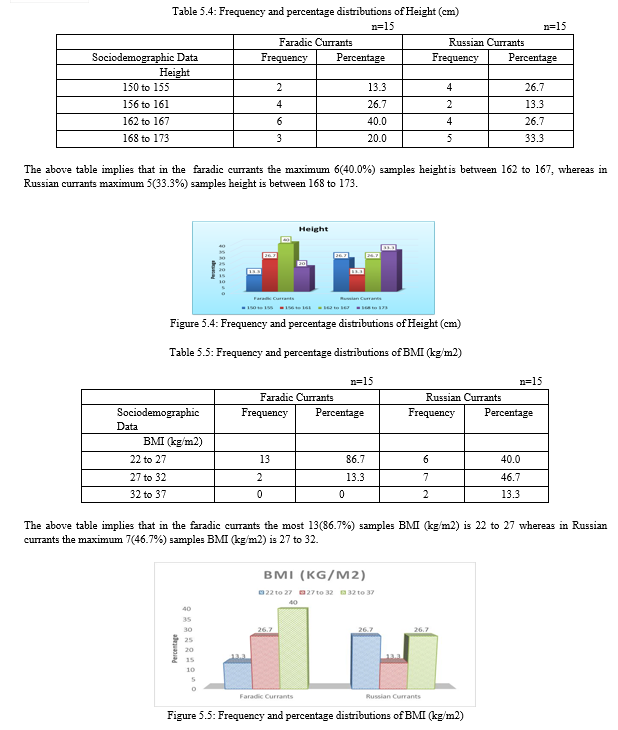
The present study shows that the maximum 8(53.3%) samples in faradic currants as well as in Russian currants are females, 7(46.7%) of the samples are males in each. In faradic currants the maximum 7(46.7%) samples are between the age 45 to 49 years, 4 (26.7%) samples are between 50 to 54 years, and the remaining 4(26.7%) samples are between 55 to 60 years. Whereas in Russian currants 5(33.3%) samples are between 45 to 49 years, another 5(33.3%) samples are between 50 to 54 years, and the remaining 5(33.3%) samples are between 55 to 60 years. In the faradic currants, the maximum 8 (%53.3) samples weight was between 60 to 68 kg, whereas in Russian currants the maximum 5 (33.3%) samples weight is between 78 to 86 kg. In the faradic currants, the maximum of 6(40.0%) samples’ height is between 162 to 167, whereas in Russian currants maximum of 5(33.3%) samples’ height is between 168 to 173. In the faradic currants, the 13(86.7%) samples’ BMI (kg/m2) is 22 to 27 whereas in Russian currants the maximum 7(46.7%) samples’ BMI (kg/m2) is 27 to 32.
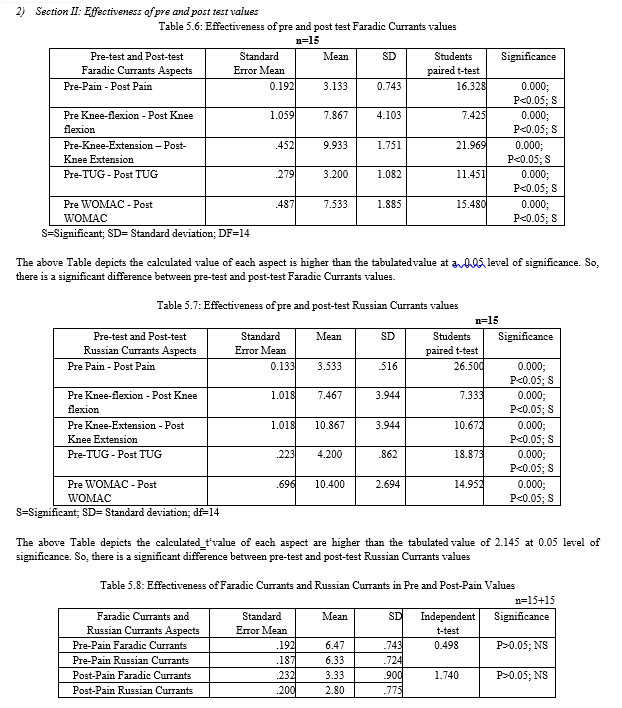
2. Section II: Effectiveness of pre and post-test values.
The present study revealed that there is a significant difference between pre-test and post-test Faradic Currants values and also there is a significant difference between pre-test and post-test Russian Currants values. It means Faradic and Russian current both are effective on quadriceps muscle in patients with knee osteoarthritis in order to increase ROM of the knee, decrease pain and improve the functional ability of the knee joint.
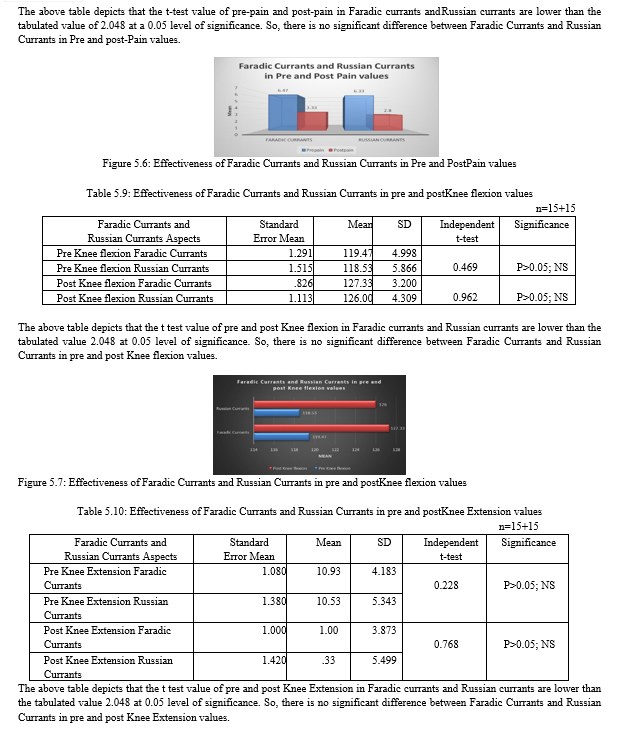
3. Section III: Comparison of Faradic Currants and Russian Currants values.
In this study, we found that there is no significant difference between Faradic Currants and Russian Currants in Pre and post Pain (NPRS) values, in pre and post Knee flexion values, pre and post Knee Extension values, in pre and post TUG values, and in pre WOMAC values (Therefore, the H0 is accepted and the H1 is rejected) but there is a significant difference between Faradic Currants and Russian Currants post WOMAC values (Therefore, the H0 is rejected and the H1 is accepted).
A study conducted by Vaz et al on neuromuscular electrical stimulation (NMES) reduces structural and functional losses of the quadriceps muscle and improves the health status of patients with knee osteoarthritis. This study concluded that the NMES strength training program was successful in counteracting the deleterious effects of OA on the knee extensor muscles. NMES reduced muscle weakness and increased muscle thickness and fascicle length. NMES training appears to offset the changes in quadriceps structure and function, as well as improve the health status of patients with knee OA [15].
The previous study conducted by Dr. Raghav s. et al to determine the comparative effect of the functional paradigm over strengthening exercises in reducing pain, joint stiffness, functional limitation, and improving isometric quadriceps muscle strength and quality of life in patients with knee osteoarthritis. This study revealed that the reduction of pain, joint stiffness, and functional limitation in both groups may be attributed to increased quadriceps muscle strength and thereby improve function which leads to decreased pain and disability. The results of this study show that the functional paradigm was an effective
Protocol for reducing pain, joint stiffness, functional limitation, and improving quadriceps muscle strength [25].
According to Ward AR et al the effect of Russian current stimulation is believed to relieve pain re-educates muscle function, prevent muscle atrophy and restore function. Russian current can cause depolarization of sensory and motor nerve fibers. It activates a fast type II motor unit and evokes muscle contraction which leads strengthening of muscle. [14]
Michael G Parker et al. conducted a study on torque responses in human quadriceps to burst modulated alternating current at 3 carrier frequencies namely, 2500 Hz, 3750, and 5000 Hz in 23 healthy subjects, and concluded that burst modulated alternating current given at 2500 Hz produces greater electrically induced torque than those generated at 3750 Hz and 5000 Hz. According to this study, we used a Russian current stimulator having 2500 Hz frequency in the present study [38].
According to a previous study, the improvement in function could be attributed to the analgesic effect of Russian current and exercises which lead to decreased pain and increase strength of the quadriceps. Strength gain was also associated with improvement in confidence during mobility [39].
Some previous studies revealed that Russian current stimulation of the peripheral muscle causes an increase in the spinal routes excitability, and changes in the cortical activation pattern, and improves the recruitment of fast twitch (fatigable) muscle fibers which are responsible for strength [40]. Also, there could be some neural adaptations that increase the capacity of voluntary muscle contraction that was impaired in patients with knee OA [41].
A study conducted by Anand B.H, Snehal R.D et al on the effect of Russian current on questions Quadriceps muscle strength with primary knee osteoarthritis.
This study concluded that the Russian current group Shows better improvement in pain an increase in muscle strength and greater improvement of the functional score (WOMAC) [26].
IX. LIMITATIONS
There are several limitations to this study. The sample size in the present study was small, No follow-up was done, the strength of the quadriceps muscle was not included, and Radio graphical findings were not measured in this study.
References
[1] Bricca A, Juhl CB, Steultjens M et al (2019) Impact of exercise on articular cartilage in people at risk of, or with established, knee osteoarthritis: a systematic review of randomised controlled trials. Br J Sports Med 53(15):940–947. https:// doi. org/10. 1136/ bjspo rts- 2017- 098661. [2] Jayant Joshi, Prakash Kotwal. Essentials of Orthopedics and Applied Physiotherapy.Elsevier Pub. 2011: 2ndedition, Chapter.16:341. [3] Kellgren, J. H.; Lawrence, J. S. (1957). Radiological Assessment of Osteo-Arthrosis.Annals of the Rheumatic Diseases, 16(4), 494–502. [4] Boon et al Davidson principle and practice of medicine, 20th edition. 2006(13): 1096-1097. [5] J .Maheshwari. Essential Orthopedics. Jaypee Brothers 2011:4thedition Chapter. 35: 287- 289. [6] E. Vignon, M. Piperno, M.P. Hellio Le Graverand, S.A. Mazzuca, et al ?Measurement of Radiographic Joint Space Width in the Tibiofemoral Compartment of the Osteoarthritic Knee. Comparison of standing anteroposterior and Lyon Schuss views.? Arthritis and Rheumatism, 48(2): 378-384, 2003. [7] Sharma MK, Swami HM, Bhatia V, et al. An epidemiological study of correlates osteoarthritis in geriatric population of UT Chandigarh. Indian J Community Med, 2007, 32: 77–78. [8] Robin McKenzie, Stephen May. The human extremities –Mechanical Diagnosis and therapy. Spinal Publication New Zealand Ltd 2007 1stedition:255 -260v [9] de Oliveira MM, Aragao FA, Vaz MA (2013) Neuromuscular electrical stimulation for muscle strengthening in elderly with knee osteoarthritis - a systematic review. Complement Ther Clin Pract 19(1):27–31. [10] Jun Iwamoto et al. Effectiveness of exercise for osteoarthritis of the knee: A review literature. World Journal of Orthopedics, 2011 May 18; 2(5):37-42. [11] Rene Calliet. Knee pain and disability. Jaypee Brothers; 3rd edition 190-197. [12] Michael V. Hurley. The role of muscle weakness in the pathogenesis of osteoarthritis Rheumatic Disease Clinics of North America, 1 May 1999; 25(2): 283-298. [13] Carolyn Kisner, Lynn Allen Colby. Therapeutic Exercise Foundations and Techniques.Jaypee Brothers 2007:5th edition. Chapter 21:691-693. [14] Ward AR, Shkuratova N. Russian electrical stimulation: the early experiments. Physical therapy. 2002 Oct 1; 82(10):1019-30. [15] Marco Aurélio Vaz et al. (2012), Neuromuscular electrical stimulation (NMES) reduces structural and functional losses of quadriceps muscle and improves health status in patients with knee osteoarthritis. Journal of Orthopaedic Research Volume 31, Issue 4: 511-516. [16] Ratan SK, Rattan KN (2009). The surged faradic faradic stimulation to the pelvic floor muscle as an adjunct to the medical management in children with rectal prolapsed, BMC pediatrics. [17] International Association for the Study of Pain (2011). Classification of Chronic Pain. Part III Pain Therms. 2. [18] Jensen, M., & McFarland, C. (1993). Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain, 55(2), 195-203. [19] Childs, J., Piva, S., & Fritz, J. (2005). Responsiveness of the Numeric Pain Rating Scale in Patients with Low Back Pain. Spine, 30(11), 1331-1334. [20] S. Jagmohan (2018), Textbook of Electrotherapy, Jaypee Brothers Medical Publishers (P) Ltd, 3rd edition, Chapter 2:75. [21] S. Jagmohan (2018), Textbook of Electrotherapy, Jaypee Brothers Medical Publishers (P) Ltd, 3rd edition, Chapter 3:134. [22] Norkin C. C., D. J. White (2016), Measurement of joint motion: a guide to goniometry, Philadelphia : F.A. Davis Company, Fifth edition, Chapter 1:7 [23] John O. Omole, Michael O. Egwu, et al (2018), Comparative Effects Of Russian Current And Isometric Resisted Exercise On Quadriceps Angle And Joint Space Width Among Patients With Primary Knee Osteoarthritis, International Journal of Advanced Research and Publications, Vol 2(2): 92-99. [24] S. Mathew et al (2020). Effectiveness of eccentric exercise and neuromuscular electrical stimulation on quadriceps function in grade II osteoarthritis- a randomized control trial, International Journal of Research and Review Vol.7; Issue: 4; 328-335 [25] Dr. Raghav S, Dr. A Singh (2020), comparative effect of the functional faradism over strengthening exercises in reducing pain, joint stiffness, functional limitation and improving isometric quadriceps muscle strength and quality of life in patients with knee osteoarthritis, International Journal of Creative Research Thoughts (IJCRT), 8(4); 2948-2956. [26] Anand B Heggannavar, Snehal R Dharmayat, Sonal S Nerurkar (2014), EFFECT OF RUSSIAN CURRENT ON QUADRICEPS MUSCLE STRENGTH IN SUBJECTS WITH PRIMARY OSTEOARTHRITIS OF KNEE: A RANDOMIZED CONTROL TRIAL. International Journal of Physiotherapy and Research, Int J Physiother Res, Vol 2(3):555- 60. [27] Rosemffet, Marcos G.; Schneeberger, Emilce E.; Citera, Gustavo, et al. (2004). Effects of Functional Electrostimulation on Pain, Muscular Strength, and Functional Capacity in Patients With Osteoarthritis of the Knee. JCR: Journal of Clinical Rheumatology, 10(5), 246–249. [28] Alghadir, Ahmad; Anwer, Shahnawaz; Brismée, Jean-Michel (2015). The reliability and minimal detectable change of Timed Up and Go test in individuals with grade 1 – 3 knee osteoarthritis. BMC Musculoskeletal Disorders, 16(1), 174–181. [29] F Salaffi; G Leardini; B Canesi; A Mannoni; A Fioravanti (2003). Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in Italian patients with osteoarthritis of the knee. , 11(8), 551–560. [30] Pratibha Prabha et al (2019). Efficacy of Russian Current on Pain, Strength of Quadriceps and Function in Subjects with Primary Knee Osteoarthritis: A Randomized Clinical Trial, International Journal of Health Sciences & Research, 9(8), 140-148. [31] John T. Farrar; Andrea B. Troxel; Colin Stott; Paul Duncombe; Mark P. Jensen (2008), Validity, reliability, and clinical importance of change in a 0—10 numeric rating scale measure of spasticity: a post hoc analysis of a randomized, double-blind, placebo- controlled trial, 30(5), 0–985. [32] Akanksha A. Nalawade, Poonam H. Patil, (2020), Comparison between Surged Faradic Current and Transcutaneous Electrical Nerve Stimulation (TENS) on Myofascial Trigger Points in Trapezius, Indian Journal of Physiotherapy and Occupational Therapy. Vol. 14, No. 1. [33] S. Epskamp et al (2020), Range of motion as an outcome measure for knee osteoarthritis interventions in clinical trials: an integrated review, Physical Therapy Reviews, 25:5-6, 462- 481. [34] Norkin C. C., D. J. White (2016), Measurement of joint motion: a guide to goniometry, Philadelphia: F.A. Davis Company, Fifth edition, Chapter 1:318-320. [35] Podsiadlo D, et al (1991). J Am Geriatr Soc. 1991; 39:142–148. [36] Shumway-Cook A, et al (2000). Phys Ther.; 80:896–903. [37] Bellamy N, Buchanan WW, Goldsmith CH, et al (1988): Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol, 15:1833-1840. [38] Michael G. Parkar et al. Torque Responses in Human Quadriceps to Burst –modulated Alternating Current at 3 Carrier Frequencies. Journal of Orthopedic and Sport Physical Therapy, April 2005; 35 (4): 239-245. [39] Van Baar ME, Assendelft WJ, Dekker J, et al. Effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a systematic review of randomized clinical trials. Arthritis Rheum. 1999; 42: 1361–1369. [40] C. Mang, J. Clair, and D. Collins, ?Neuromuscular electrical stimulation has a global effect on corticospinal excitability for leg muscles and a focused effect for hand muscles.? Experimental Brain Research, 209(3): 355-363, 2011. [41] S.C. Petterson, P. Barrance, T. Buchanan, et al, ?Mechanisms underlying quadriceps weakness in knee osteoarthritis.? Medicine and Science in Sports and Exercise, 40(3):422- 427, 2008.
Copyright
Copyright © 2023 Neha Rani, Sonam Verma, Karishma Das, Palas Pramanick, Komal Chauhan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Download Paper
Paper Id : IJRASET55301
Publish Date : 2023-08-12
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here